GLP-1 vs GLP-3: Unraveling the Molecular Edge in Metabolic Medicine
GLP-1 vs GLP-3: Unraveling the Molecular Edge in Metabolic Medicine
At the forefront of diabetes and obesity research, GLP-1 and GLP-3 hormones represent two distinct yet related peptide players with growing influence over metabolic health. While GLP-1 (glucagon-like peptide-1) is widely recognized as a key therapeutic target, GLP-3—less studied but increasingly scrutinized—carries emerging implications for glucose regulation and appetite control. Understanding the differences between GLP-1 and GLP-3 is essential for researchers, clinicians, and patients navigating next-generation metabolic treatments.
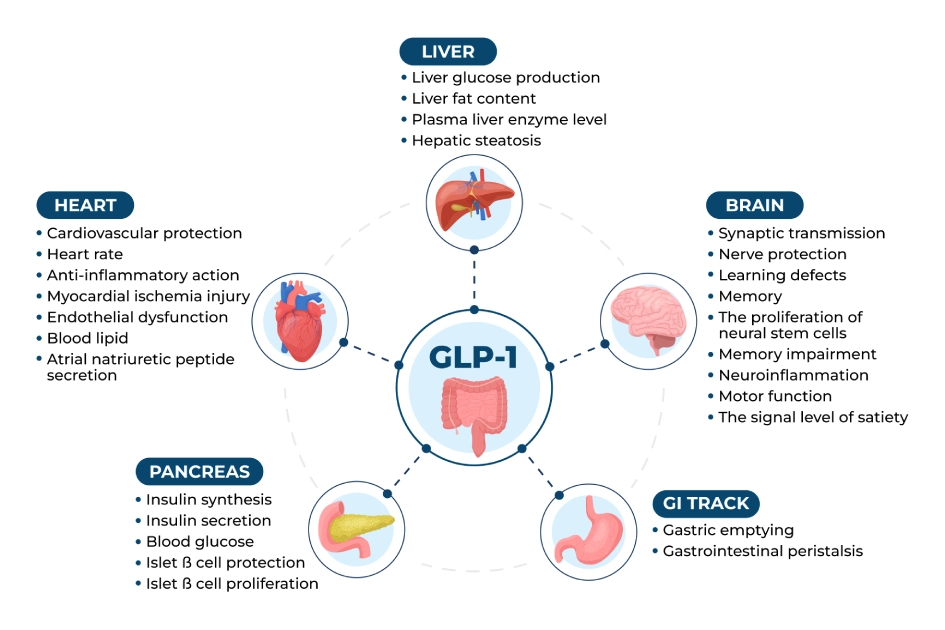
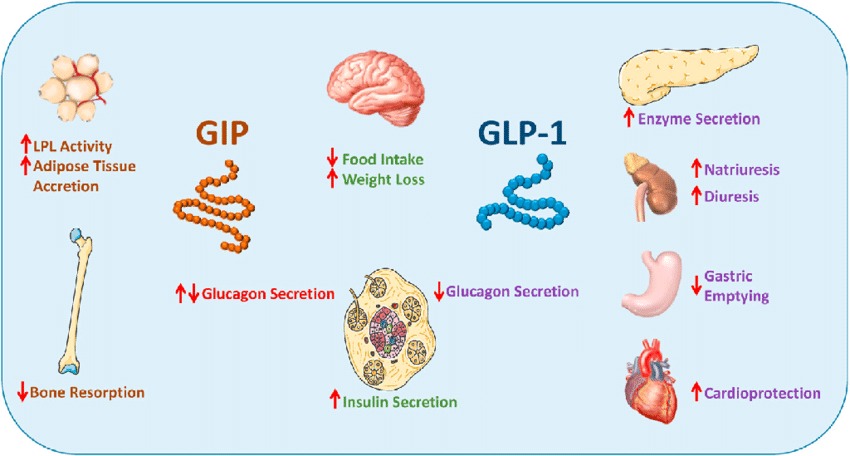
GLP-1, a 30-amino-acid peptide derived from proglucagon, is best known for stimulating insulin secretion in response to rising blood glucose levels. Unlike many short-acting incretins, GLP-1 triggers insulin release only when glucose is elevated, reducing hypoglycemia risk—a critical advantage in diabetes therapy. Beyond glycemic control, GLP-1 suppresses glucagon secretion, slows gastric emptying, and promotes satiety via central nervous system signaling.
“Its multifunctional action makes GLP-1 one of the most potent secretagogues available,” notes Dr. Elena Park, an endocrinologist at the Metabolic Health Institute. “The drug class it launched—GLP-1 receptor agonists—has transformed type 2 diabetes care and expanded into weight management.”
GLP-1: The Gold Standard in Metabolic Therapeutics
GLP-1’s clinical impact is rooted in robust evidence from both preclinical models and human trials.Its role in lowering HbA1c, reducing cardiovascular risk, and supporting sustained weight loss through appetite suppression underpins its widespread adoption.
- Mechanism: GLP-1 binds to GLP-1 receptors on pancreatic beta cells, activating adenylate cyclase and elevating cAMP, which amplifies glucose-dependent insulin release.
- Delivery Challenges: Naturally cleaved rapidly by dipeptidyl peptidase-4 (DPP-4), limiting oral efficacy. This constraint drove development of modified analogs and sustained-release formulations.
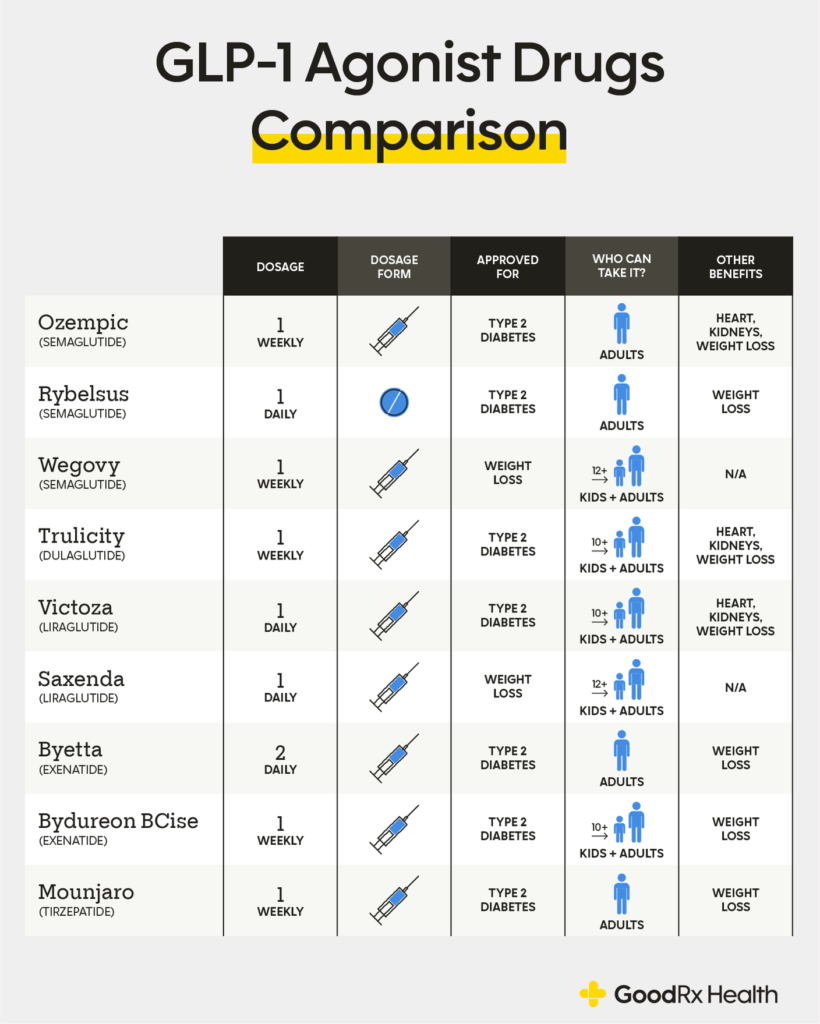
- Broad Applications: Approved for type 2 diabetes (e.g., semaglutide, liraglutide) and obesity (e.g., semaglutide 2.4 mg).
Indexed for long-term reduction in major adverse cardiovascular events (MACE).
In contrast, GLP-3—structurally similar but functionally distinct—has emerged as a lesser-known yet promising analog. Though not as extensively studied, GLP-3 peptides share the glucagon-like scaffold but exhibit altered receptor selectivity and metabolic effects.
GLP-3: The Emerging Player in Metabolic Regulation
GLP-3, a 31-amino-acid analog derived from proglucagon, shares 85% amino acid identity with GLP-1 but differs in key functional domains.While less characterized, early research suggests unique biological activity, particularly in appetite modulation and glucose stabilization.
GLP-3’s primary distinction lies in its preferred signaling pathway activation. Unlike GLP-1, which robustly stimulates insulin secretion and cAMP pathways, GLP-3 appears to preferentially engage GLP-1 receptor variants linked to satiety centers in the hypothalamus.
This selective action may offer nuanced control over feeding behavior without compromising insulin response. Preliminary animal studies in obese rodent models show GLP-3 reduces food intake more selectively and enhances hepatic glycogen storage, suggesting potential benefits in glucose homeostasis independent of insulin spikes.
Mechanistic Divergence: Signal Pathways and Receptor Dynamics
The divergent effects of GLP-1 and GLP-3 stem largely from subtle differences in receptor interaction. GLP-1 activates both GLP-1R and GLP-2R, driving insulin secretion and gut mucosal improvements.GLP-3 exhibits higher affinity for GLP-1R isoforms linked to central appetite suppression, potentially explaining its appetite-regulating effects independent of robust insulinotropic activity. “GLP-3 may act like a ‘smart interface’—influencing metabolism while avoiding overstimulation of insulin release,” explains Dr. James Chen, a molecular endocrinologist specializing in peptide therapeutics.
“This could address a major limitation of first- and second-generation GLP-1 agonists: episodes of hypoglycemia and unpredictable satiety responses.”
Clinical Trajectory and Research Frontiers
As of now, GLP-3 remains primarily confined to basic science and preclinical development. No commercial agents targeting GLP-3 are approved, though several biotech firms are exploring its therapeutic potential. Early trials in metabolic syndrome models indicate GLP-3 improves insulin sensitivity and reduces epicentral fat deposition—areas where GLP-1 has shown less precision.“GLP-3 isn’t a replacement but a refinement,” notes Dr. Park. “Its unique receptor bias suggests tailored use in patients requiring targeted appetite control without pronounced insulin effects—possibly in secondary obesity or specific diabetes phenotypes.”
Differences extend to pharmacokinetics: GLP-3 peptides, engineered for enhanced receptor selectivity, potentially offer prolonged action with lower dose frequency.
This contrasts with GLP-1 analogs, where frequent dosing is often required to maintain efficacy due to rapid degradation. Such improvements could enhance patient adherence and reduce side effects like nausea, a major barrier to long-term use.
Challenges and Regulatory Pathways
Despite its promise, GLP-3 faces significant hurdles.Limited clinical data restricts regulatory approval pathways, and skepticism persists due to GLP-1’s voluminous validation. Establishing safety profiles in larger populations remains a priority, particularly regarding renal and cardiovascular outcomes.

Related Post

South Orange Blossom Trail: Where Spring Blossoms Meet Urban Vitality
From Frieren’s Fierce Lineage: The Hidden Strength Behind the Valkyrian Dragons

Unlocking Tilly Discovery: Mapping the Hidden Mysteries of Physical & Digital Exploration
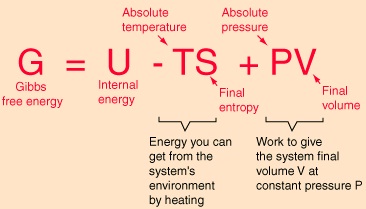
Unlocking Clean Energy: The Science Behind Water Electrolysis and Gibbs Free Energy